Hammer Toe Pain Treatment Options
 Overview
Overview
The smallest four toes of each foot have three bony segments connected by two joints. Hammertoe is a deformity in which one or more of the small toes develops a bend at the joint between the first and second segments. The tip of the toe turns downward, making it look like a hammer or claw. The second toe is the one most often affected. Hammer toe may be more likely to occur when the second toe is longer than the first toe or when the arch of the foot is flat.
Causes
Hammer toes are most frequently caused by a muscle - tendon imbalance in the foot, and are seen both in adults and children. Foot muscles work in pairs to straighten and bend the toes. If your foot has a biomechanical defect, the muscles tighten and the tendons shorten. Eventually, the toe muscles can?t straighten the toe, even when barefoot. Contributing factors are poor choices in footwear, arthritis, or trauma.
 Symptoms
Symptoms
People who have painful hammertoes visit their podiatrist because their affected toe is either rubbing on the end their shoe (signaling a contracted flexor tendon), rubbing on the top of their shoe (signaling a contracted extensor tendon), or rubbing on another toe and causing a painful buildup of thick skin, known as a corn.
Diagnosis
The exam may reveal a toe in which the near bone of the toe (proximal phalanx) is angled upward and the middle bone of the toe points in the opposite direction (plantar flexed). Toes may appear crooked or rotated. The involved joint may be painful when moved, or stiff. There may be areas of thickened skin (corns or calluses) on top of or between the toes, a callus may also be observed at the tip of the affected toe beneath the toenail. An attempt to passively correct the deformity will help elucidate the best treatment option as the examiner determines whether the toe is still flexible or not. It is advisable to assess palpable pulses, since their presence is associated with a good prognosis for healing after surgery. X-rays will demonstrate the contractures of the involved joints, as well as possible arthritic changes and bone enlargements (exostoses, spurs). X-rays of the involved foot are usually performed in a weight-bearing position.
Non Surgical Treatment
Conservative treatment starts with new shoes that have soft, roomy toe boxes. Shoes should be one-half inch longer than your longest toe. (Note: For many people, the second toe is longer than the big toe.) Avoid wearing tight, narrow, high-heeled shoes. You may also be able to find a shoe with a deep toe box that accommodates the hammer toe. Or, a shoe specialist (Pedorthist) may be able to stretch the toe box so that it bulges out around the toe. Sandals may help, as long as they do not pinch or rub other areas of the foot.
Surgical Treatment
If a person's toes have become very inflexible and unresponsive to non-invasive means of treatment and if open sores have developed as a result of constant hammertoes friction, they may receive orthopaedic surgery to correct the deformity. The operation is quick and is commonly performed as an out-patient procedure. The doctor administers a local anesthetic into the person's foot to numb the site of the operation. The person may remain conscious as the surgeon performs the procedure. A sedative might also be administered to help calm the person if they are too anxious.
 Prevention
Prevention
In addition to wearing proper shoes and socks, walking often and properly can prevent foot injury and pain. The head should be erect, the back straight, and the arms relaxed and swinging freely at the side. Step out on the heel, move forward with the weight on the outside of the foot, and complete the step by pushing off the big toe. Exercises specifically for the toe and feet are easy to perform and help strengthen them and keep them flexible. Helpful exercises include the following. Raise and curl the toes 10 times, holding each position for a count of five. Put a rubber band around both big toes and pull the feet away from each other. Count to five. Repeat 10 times. Pick up a towel with the toes. Repeat five times. Pump the foot up and down to stretch the calf and shin muscles. Perform for 2 or 3 minutes.
Discover More About Overpronation
Overview
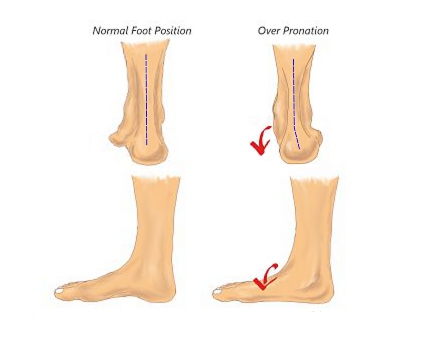
When the ankles over-pronate, it throws everything out of alignment. The bones in the feet can actually shift over time, and the muscles and tendons in the leg and ankle will twist. This places repetitive stress on the ligaments, tendons, joints and muscles of the foot, which can cause injury. If your feet are over-pronating, you may notice your muscles feet unusually tired when you way or stand, or they may ache. But symptoms will vary by your weight, age and activity.
Causes
During our development, the muscles, ligaments, and other soft tissue structures that hold our bones together at the joints become looser than normal. When the bones are not held tightly in place, the joints are not aligned properly, and the foot gradually turns outward at the ankle, causing the inner ankle bone to appear more prominent. The foot moves in this direction because it is the path of least resistance. It is more difficult for the foot to move in the opposite direction (this is called supination). As we develop, the muscles and ligaments accommodate to this abnormal alignment. By the time growth is complete, the pronated foot is: abnormally flexible, flat, and its outer border appears raised so that as you step down you do not come down equally across the entire foot; instead, you come down mostly on the inner border of the foot. Normal aging will produce further laxity of our muscles that causes the pronation to become gradually worse.
Symptoms
With over pronation, sufferers are most likely to experience pain through the arch of the foot. A lack of stability is also a common complaint. Over pronation also causes the foot to turn outward during movement at the ankle, causing sufferers to walk along the inner portion of the foot. This not only can deliver serious pain through the heel and ankle, but it can also be the cause of pain in the knees or lower back as well. This condition also causes the arch to sink which places stress on the bones, ligaments, and tendons throughout the foot. This may yield other common conditions of foot pain such as plantar fasciitis and heel spurs.
Diagnosis
People who overpronate have flat feet or collapsed arches. You can tell whether you overpronate by wetting your feet and standing on a dry, flat surface. If your footprint looks complete, you probably overpronate. Another way to determine whether you have this condition is to simply look at your feet when you stand. If there is no arch on the innermost part of your sole, and it touches the floor, you likely overpronate. The only way to truly know for sure, however, is to be properly diagnosed by a foot and ankle specialist.

Non Surgical Treatment
Over-Pronation can be treated conservatively (non-surgical treatments) with over-the-counter orthotics. These orthotics should be designed with appropriate arch support and medial rearfoot posting to prevent the over-pronation. Footwear should also be examined to ensure there is a proper fit. Footwear with a firm heel counter is often recommended for extra support and stability. Improper fitting footwear can lead to additional problems of the foot.
Prevention
Massage and stretch the calves to increase dorsiflexion at the foot/ankle. Dorsiflexion is the bending at the ankle. By improving the dorsiflexion, one will have more flexibility at the ankle, which will allow the foot to over-pronate less. Massage the IT Band with a foam roller or tennis ball to quiet down the tightness throughout this part of the leg. The IT Band attaches from the glute maximus and runs down the side of the leg into the knee area. When the IT Band is tight it will accelerate the force of the leg moving inward, which will cause the foot to move inward as well. It is often that tightness through the IT Band that promotes over-pronation. Decreasing over-pronation, which is very prominent in runners, will help add endurance, speed and efficiency to your run and ultimately place less stress on your body.
All The Things You Should Understand About Heel Pain
Overview

Heel pain is most often caused by plantar fasciitis, a condition that is sometimes also called heel spur syndrome when a spur is present. Heel Pain may also be due to other causes, such as a stress fracture, tendonitis, arthritis, nerve irritation, or rarely, a cyst. Because there are several potential causes, it is important to have heel pain properly diagnosed. A foot and ankle surgeon is able to distinguish between all the possibilities and determine the underlying source of your heel pain.
Causes
The most common cause of heel pain is a pull on the heel bone exerted by the muscles and ligaments (plantar fascia shown in illustration above) that support the arch of the foot. This is an overuse condition similar to bursitis of the shoulder or tennis elbow. Plantar fasciitis is typically very painful in the morning during the first few steps, after sitting and again at the end of the day.
Symptoms
Usually worse with the first few steps in the morning or at the initial point of activity. The latter usually gets better with continued activity (squeaky hinge analogy). Walking, running, sprinting, hill running and jumping will increase the pain. Often, the natural response is to walk on the outside of the foot - in supination - to lessen the stress on the plantar fascia - resulting in new problems.
Diagnosis
Depending on the condition, the cause of heel pain is diagnosed using a number of tests, including medical history, physical examination, including examination of joints and muscles of the foot and leg, X-rays.
Non Surgical Treatment
Calf stretch, silicone Heel cups, ice, night splint, physical therapy. Sometimes custom orthotics are beneficial in long standing cases. Steroid injections have been used and although they temporarily relieve the pain, the pain usually returns within a short period of time. Plantar fasciitis tends to go away in 90% of all people in time. It can take 12-18 months for all the pain to resolve. If the pain continues after adequate treatment, high frequency shock wave therapy (OssaTron) has been found to be beneficial, unfortunately most insurance companies do not cover this procedure.
Surgical Treatment
Although most patients with plantar fasciitis respond to non-surgical treatment, a small percentage of patients may require surgery. If, after several months of non-surgical treatment, you continue to have heel pain, surgery will be considered. Your foot and ankle surgeon will discuss the surgical options with you and determine which approach would be most beneficial for you. No matter what kind of treatment you undergo for plantar fasciitis, the underlying causes that led to this condition may remain. Therefore, you will need to continue with preventive measures. Wearing supportive shoes, stretching, and using custom orthotic devices are the mainstay of long-term treatment for plantar fasciitis.
Prevention

Make sure you wear appropriate supportive shoes. Don't over-train in sports. Make sure you warm up, cool down and undertake an exercise regime that helps maintain flexibility. Manage your weight, obesity is a factor in causing plantar fasciitis. Avoid walking and running on hard surfaces if you are prone to pain. You should follow the recognized management protocol "RICED" rest, ice, compression, elevation and diagnosis. Rest, keep off the injured ankle as much as possible. Ice, applied for 20 minutes at a time every hour as long as swelling persists. Compression, support the ankle and foot with a firmly (not tightly) wrapped elastic bandage. Elevation, keep foot above heart level to minimize bruising and swelling. Diagnosis. Consult a medical professional (such as a Podiatrist or doctor) especially if you are worried about the injury, or if the pain or swelling gets worse. If the pain or swelling has not gone down significantly within 48 hours, also seek treatment. An accurate diagnosis is essential for proper rehabilitation of moderate to severe injuries.